Dog-Mediated Rabies Exposure to Humans in Ethiopia: A Systematic Review and Meta-analysis
1Health Research Development Directorate, Amhara Public Health Institute, Bahir Dar, Ethiopia
2Bahir Dar University, Bahir Dar, Amhara, Ethiopia
3Durbete Primary Hospital, Durbete, Amhara, Ethiopia
*Corresponding Author: e-mail gizew.dessie@gmail.com, ORCID: https://orcid.org/0000-0002-3979-3998
Background: Dog-mediated rabies is a global public health agenda, especially in developing countries like in Asia and Africa. More than 95% of rabies incidence can be reduced by dog vaccination coverage of 70 %. In Ethiopia, a review of facility-based studies indicated around 32 % of dog-mediated human rabies exposure cases, which seems low compared to the global estimate. Given this finding, assessing comprehensive level of human exposure to dog-mediated rabies in Ethiopia becomes a crucial first step toward addressing the issue. Therefore, this review aimed to pool the prevalence of dog-mediated rabies exposure to humans using both community and facility-level studies.
Methods: We prepared a review protocol per Joanna Briggs Institute (JBI) manual for evidence synthesis and conducted a comprehensive search of PubMed, Cochrane, Google Scholar, and African Index Medicus databases and grey literature from 17 December 2023 to 06 April 2024. The pooled prevalence of dog-mediated rabies exposure to humans was computed using R v 4.3.1 software. Subgroup analysis was done on sample size, geographical location, and year of publication. Publication bias was assessed using a funnel plot.
Results: Based on 21 studies and 9,261 participants, the pooled prevalence of dog-mediated rabies exposure to humans was 90% (95% CI: 83-94) for the random effects model with I2 = 97% and p < 0.01. Sub-group analysis was done to investigate the source of heterogeneity, including sample size, study area, and year of publication. All the above-listed variables were not significant sources of statistical heterogeneity.
Conclusion and recommendations: This finding showed that the prevalence of dog mediated rabies exposure to humans is high. Therefore, the Ethiopian ministry of health, in collaboration with animal health, through a one-health approach, should target dog management including vaccination to preventive coverage (70%) to prevent the risk of rabies by dogs.
Keywords: dog-mediated; Ethiopia; humans; prevalence; rabies exposure
የጥናቱ ዳራ፡-የእብድ ውሻ በሽታ ዓለም አቀፍ የህበረተሰብ ጤና አጀንዳ ሲሆን በአፍሪካ እና በኤስያ ሀገራት ችግሩ የባሰ ነው። ከ 95% በላይ የሚሆነውን የእብድ ውሻ በሽታ 70% ውሾችን በማስከተብ መከላክል እንደሚቻል ጥናቶች ያሳያሉ። በኢትዮጵያ የጤና ተቋማትን መረጃ መሰረት ተደርገው የተሰሩ ጥናቶች እንደሚያሳዩት በእብድ ውሻ በሽታ የተጋለጡት 32% ይደርሳሉ። ይህ አሀዝ ከዓለም አቀፈ የተጋላጭነት ግምት ሲታይ ዝቅ ያለ ይመስላል። ይህን መረጃ መሰረት በማድረግ እና በማህበረሰብ ደረጃ የተጠኑ ጥናቶችን በመጠቀም በሀገር ደረጃ ወካይ የሆነ እና ለትግበራ በቂ አቅጣጫ የሚሰጥ ጥናት በቅድሚያ ያስፈልጋል።
የጥናቱ ዓላማ፡- የዚህ ጥናት ዓላማ በጤና ተቋማት እና በማህበረሰብ ደረጃ የተጠኑ ጥናቶችን በመጭመቅ የእብድ ዉሻ በሸታ ተጋላጭነት በኢትዮጵያ ምን ያህል እንደሆነ ማሳየት ነው።
የጥናቱ ዘዴ፡- ይህ ጥናት የጆዋና ብሪግስ ኢነስቲትዩት ፕሮቶኮልን በመጠቀም ሂደቱ የተከናወነ ሲሆን መረጃዎችም ከPubMed, Cochrane, Google Scholar, and African Index Medicus የመረጃ ቋቶች እና ያልታተሙ መረጃዎችን ጨምሮ እኤአ ከ17/12/ 2023 እስከ 06 /04/ 2024 መረጃው ተሰብስቡዋል። መረጃ ለመትንትን R v 4.3.1 software በመጠቀም ተሰርቱዋል። ውጤቱም በተጠኑበት አካባቢ፥ በተጠኑበት ጊዜ እና በጥናቱ ተሳታፊዎች ብዛት መሰረት ተደርጎ ትንተና ተደርጉዋል። የጥናቶቹ ትክክለኛነት ፈነል ፕሎትን በመጠቀም ተረጋግጡዋል።
የጥናቱ ውጤት፡- በ 21 ጥናቶች እና በ 9,261 ተሳታፊዎች መሰረት የእብድ ውሻ በሽታ ተጋላጭነት በኢትዮጵያ 90% ይደርሳል። የተጠኑበት አካባቢ፥ የተጠኑበት ጊዜ እና የጥናቱ ተሳታፊዎች ብዛት በውጤቱ የጎላ ልዩነት ኣላሳዩም።
የጥናቱ ማጠቃለያ ና ምክረሃሳብ፡- የዚህ ጥናት ግኝት እንደሚያሳየው የእብድ ውሻ በሽታ ተጋላጭነት በኢትዮጵያ ከፍተኛ ነው። በተቀናጀ ሁኔታ የውሻ አያያዝን ክትባትን ጨምሮ በማሻሻል ችግሩን መፍታት አስፈላጊ ነው።
ቁልፍ ቃላት-ኢትዮጵያ; የእብድ ውሻ በሽታ ተጋላጭነት፤ ከውሻ ጋር የተያያዘ ሬቢስ
Rabies is a zoonotic disease that is caused by a single-stranded RNA virus belonging to the family Rhabdoviridae. This virus possesses a non-segmented, negative-sense genome. The incubation period of rabies can vary significantly, ranging from a few days to more than a year, it commonly lasts between 20 to 90 days (1).
The transmission of the rabies virus occurs primarily through direct contact involving broken skin due to bite or mucous membranes in the eyes, nose, or mouth with saliva or brain/nervous system tissue from an infected animal. Typically, individuals contract rabies from the bite of a rabid animal. However, although uncommon, it is also possible for individuals to acquire rabies through non-bite exposures, including scratches, abrasions, or open wounds that come into contact with saliva or other potentially infectious materials from a rabid animal (2).
Rabies has a global distribution, being prevalent on all continents except Antarctica. Currently, it contributes to over 59,000 human fatalities annually, with approximately 40% of these deaths occurring among children. The majority of rabies cases, exceeding 80%, are concentrated in impoverished rural areas of Africa and Asia, where access to medical and veterinary services is limited (3). The impact of rabies extends with an estimated burden of 3.7 million disability-adjusted life years (DALYs) and a total economic losses of 8.6 billion USD annually worldwide (4). Rabies, despite being preventable, is nearly 100% fatal once it progresses to symptomatic acute encephalitis. It affects nearly all mammalian species, and transmission to humans occurs primarily through bite of rabid mammals such as dogs, cats, and foxes. Among these vectors, dogs are the most significant worldwide, accounting for approximately 99% of human rabies cases (5).
In Africa, approximately 21,476 human fatalities are attributed to dog-mediated rabies annually, translating to an alarming rate of three deaths per hour. By implementing comprehensive awareness campaigns, attaining a minimum of 70% vaccination coverage among dogs, and enhancing access to post-exposure prophylaxis (PEP), a significant number of lives can be saved (6).
Rabies remains a significant public health challenge in Ethiopia, with the country registering one of the highest rabies mortality rates globally, resulting in over 2,700 human deaths annually, equivalent to approximately eight deaths per day. The economic impact is substantial, estimated at US$ 114,881,471 per year. However, due to underreporting and limited diagnostic facilities, the exact number of rabies-related deaths is uncertain. Moreover, access to life-saving human rabies post-exposure prophylaxis (PEP) is limited across the country (7,8).
There are limited studies on dog-mediated human rabies cases (9) and no comprehensive studies on dog-mediated rabies exposure to humans as rabies exposure information is very important to act than rabies cases which is not manageable once it become symptomatic. Despite the known burden, there is a lack of comprehensive data on the prevalence of human exposure to dog-mediated rabies , a critical early indicator for prevention. Measuring exposure, rather than only confirmed cases, is essential because rabies is nearly always fatal once clinical symptoms appear. Thus, this review aimed to pool the prevalence of human rabies exposure by dogs in Ethiopia for evidence-based recommendations.
To pool the prevalence of dog mediated rabies exposure to humans in Ethiopia
A systematic review and meta-analysis using condition, context and population (COCOPOp) framework based on PRISMA guidelines were done to assess the prevalence of dog-mediated human rabies exposure in Ethiopia. We conducted a comprehensive search of articles using PubMed, Cochrane, Google Scholar and African Index Medicus databases and grey literature like the WHO library. The search was conducted from 17 December 2023 to 06 April 2024. The following were searching strings used for PubMed search and were modified accordingly for other databases: rabies OR (rabies Virus) OR (rabies disease) AND expos* OR victims OR suspected AND patients OR individuals OR clients OR human AND (dog mediated) AND prevalence OR proportion AND Ethiopia.
The inclusion criteria were based on COPOPOp fromework
Table 1 Inclusion and exclusion criteria of articles
| Included studies |
Excluded studies |
|---|---|
| 1. Rabies studies that assessed source of rabies exposure in Ethiopia using any design, setting, and any time | 1. Rabies exposure studies that do not assess sources of exposure. |
| 2. Studies written in English language | 2. Experimental studies on rabies virus pathogenesis, vaccine trial and diagnosis. |
| 3. Rabies exposure studies that have no full text access. |
The screening process conducted in two stages using EndNote v. 20. Initially, papers were screened using titles and abstracts. In level two, papers that passed the initial screening were retrieved and assessed against the eligibility criteria by reading the full text. All chosen articles from this stage were stored in a designated folder for methodological quality evaluation, and their level of quality were included in this evidence synthesis. Excluded papers from the full-text assessment were justified at the PRISMA flow diagram based on the inclusion and exclusion criteria. The entire screening and selection process was carried out independently by two authors, who subsequently compared their findings and resolved minor discrepancies through consensus.
A JBI critical appraisal tool based on the study design was utilized to evaluate the methodological quality of the studies (refer to Annex 1) was employed in this study. Two independent reviewers, GDA and YKG, assessed the studies using this tool. The checklist comprised 9 criteria for rating various quality elements. And the level of methodological quality for each paper was rated by reviewers and their disagreements during rating were resolved through consensus.
The extraction of data was conducted using a template provided by JBI, ensuring uniformity in data collection across all included studies. Both reviewers, GDA and YKG, independently extracted the required data, covering aspects such as study details, methodology, and results.
Narrative summary in this systematic review utilized tables, graphs, and other diagrams to compare the characteristics (publication year, geographical location, sampl size, study design) of each included study. Pooling of the quantitative results were done under R software using random effects model at 95% confidence level. The extent of heterogeneity across studies was checked using the Q-test (p-value < 0.05) and I²-test (I squared >50% indicating significant heterogeneity). Subgroup analysis was conducted to explore the sources of heterogeneity across studies using sample size, geographical location and publication time
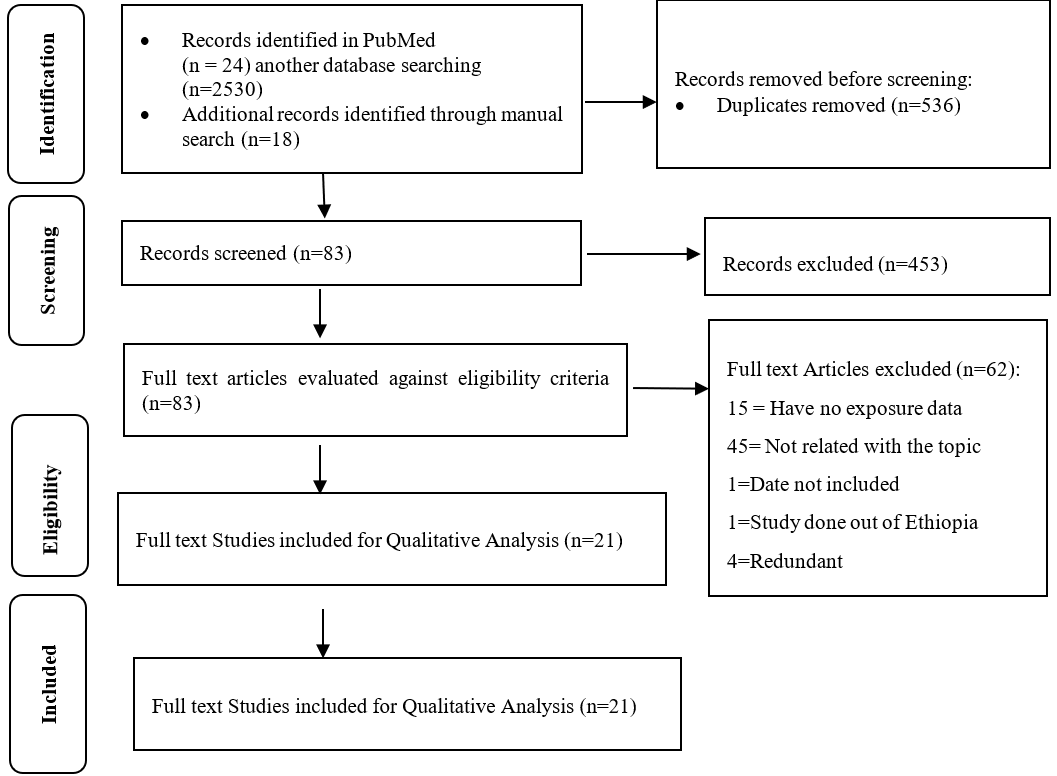
During the bibliographic database search, a total of 2,572 studies were initially identified. Following the removal of duplicates, which accounted for 2,036 studies, 536 studies remained. Upon screening the titles and abstracts, 453 studies were found unrelated and excluded. Subsequently, 83 full-text articles were retrieved for further evaluation against the eligibility criteria, out of which 15 were excluded as they did not include data on the source of exposure for human rabies. Additionally, 45 full-text articles were found to be unrelated to the objectives of this systematic review and were excluded. One article was excluded due to its publication date, and another article was excluded because of the study location being outside Ethiopia. Ultimately, 21 full-text articles were included for evidence synthesis (Fig 1).
Figure 1 Flowchart presenting the study selection with the Preferred Reporting Items for systematic Review and Meta analysis (PRISMA).
Among 21 included studies published from 2013-2023 in Ethiopia, the smallest sample size was 107 on a study done in Oromia and the largest one was 1440 on a study done in Tigray regional state. The study settings included were at community level except single study done at health facilities in Oromia. These studies involved a total of 9,261 participants (Table 2).
Table 2 Characteristics of included studies
| Study_ID | Publication year | Study | Study Setting | Study Design | Sample Size | Exposed by | |
|---|---|---|---|---|---|---|---|
| Location | Dog | Others | |||||
| Tadesse_2014(10) | 2014 | Amhara | Community | Cs | 410 | 293 | 117 |
| Ebuy_2019(11) | 2019 | Tigray | Community | Cs | 1440 | 1041 | 399 |
| Awoke_2015(12) | 2016 | Amhara | Community | Cs | 384 | 280 | 104 |
| Nigatu_2016(13) | 2016 | Amhara | Community | Cs | 416 | 363 | 53 |
| Nejash_2017(14) | 2017 | Oromia | Community | Cs | 135 | 83 | 52 |
| Tariku_2017(15) | 2017 | Oromia | Community | Cs | 384 | 374 | 10 |
| Addis_2019(16) | 2019 | Amhara | Community | Cs | 384 | 317 | 67 |
| Yigardush_2017(17) | 2017 | Amhara | Community | Cs | 360 | 248 | 112 |
| Eyob_2016(18) | 2016 | Addis_Ababa | Community | Cs | 384 | 299 | 85 |
| Adane_2022(19) | 2022 | Amhara | Community | Cs | 899 | 799 | 100 |
| Amare_2020(20) | 2020 | Amhara | Community | Cs | 384 | 273 | 111 |
| Haben_2020(21) | 2020 | Tigray | Community | Cs | 399 | 333 | 66 |
| Shumye_2016(22) | 2016 | Amhara | Community | Cs | 139 | 136 | 3 |
| Tadele_2015(23) | 2015 | Oromia | Health Facility | Cs | 384 | 380 | 4 |
| Hunde_2023(24) | 2023 | Oromia | Community | Cs | 384 | 226 | 158 |
| Tamiru_2017(25) | 2017 | Oromia | Community | Cs | 406 | 371 | 35 |
| Reta_2015(26) | 2015 | Amhara | Community | Cs | 400 | 397 | 3 |
| Tsegaye_2016(27) | 2016 | Oromia | Community | Cs | 803 | 775 | 28 |
| Balako_2019(28) | 2019 | Oromia | Community | Cs | 107 | 96 | 11 |
| Wudu_2013(29) | 2013 | Amhara | Community | Cs | 120 | 118 | 2 |
| Rea_2016(30) | 2016 | Oromia | Community | Cs | 539 | 539 | 0 |
| Total | 9261 | 7741 | 1520 | ||||
Methodological quality assessment was done using the JBI’s Prevalence Studies Critical Appraisal Checklist. Assessment was done by two independent assessors, GDA and YKG. Discrepancies between assessors were resolved through consensus and mutual understanding. The assessment results revealed that methodological quality of included studies ranged from 66.7% to 100% (Table 3).
Table 3 Methodological quality of included studies, 2023
| Study ID | Was the sample frame appropriate to address the target population?(1) | Were study participants sampled in an appropriate way?(2) | Was the sample size adequate?(3) | Were the study subjects and the setting described in detail?(4) | Was the data analysis conducted with sufficient coverage of the identified sample?(5) | Were valid methods used for the identification of the condition?(6) | Was the condition measured in a standard, reliable way for all participants?(7) | Was there appropriate statistical analysis?(8) | Was the response rate adequate, and if not, was the low response rate managed appropriately?(9) | Total Yes/comment |
|---|---|---|---|---|---|---|---|---|---|---|
| Tadesse_2014 | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | 88.90% |
| Ebuy_2019 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 100% |
| Awoke_2015 | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 88.90% |
| Nigatu_2016 | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | 88.90% |
| Nejash_2017 | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 77.80% |
| Tariku_2017 | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 88.90% |
| Addis_2019 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 88.90% |
| Yigardush_2017 | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | 77.80% |
| Eyob_2016 | No | Yes | No | Yes | No | Yes | Yes | Yes | Yes | 66.70% |
| Adane_2022 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 100% |
| Amare_2020 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 100% |
| Haben_2020 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 88.90% |
| Shumye_2016 | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 77.80% |
| Tadele_2015 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 100% |
| Hunde_2023 | No | Yes | Yes | No | Yes | No | Yes | Yes | Yes | 66.70% |
| Tamiru_2017 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 100% |
| Reta_2015 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 100% |
| Tsegaye_2016 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 100% |
| Balako_2019 | No | Yes | No | Yes | No | Yes | Yes | Yes | Yes | 66.70% |
| Wudu_2013 | No | Yes | No | Yes | Yes | Yes | No | Yes | Yes | 66.70% |
| Rea_2016 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 100% |
The pooled prevalence of human rabies due to exposure to dogs was 90% (95% CI:83 - 94) for the random effects model with I2 =97% and p<0.01 (Fig 2)
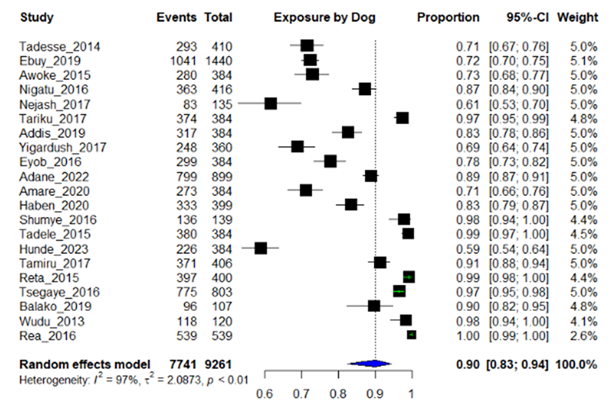
Figure 2 Forest plot showing dog mediated rabies exposure to humans
The funnel plot below indicates that there is no asymmetry in the distribution of effect sizes. This funnel plot shows that there is no publication bias for included studies (Fig 3).
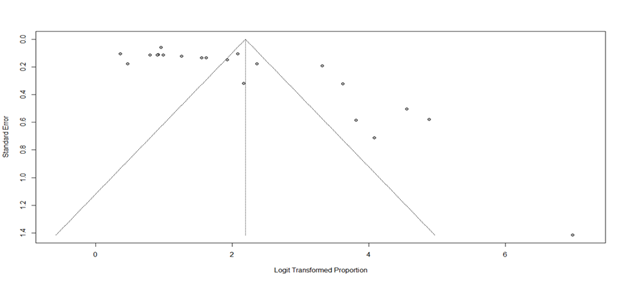
Figure 3 Funnel plot of included studies for dog mediated rabies exposure to humans
To investigate source of heterogeneity, sub group analysis was done on sample size, study area, and year of publication. Year of publication (I2=97%, p<0.01), Study location (I2=96-99 %, p<0.01) and study sample size >500 (I2=93-97%, p<0.01) were the source of heterogeneity (Fig 4-6).
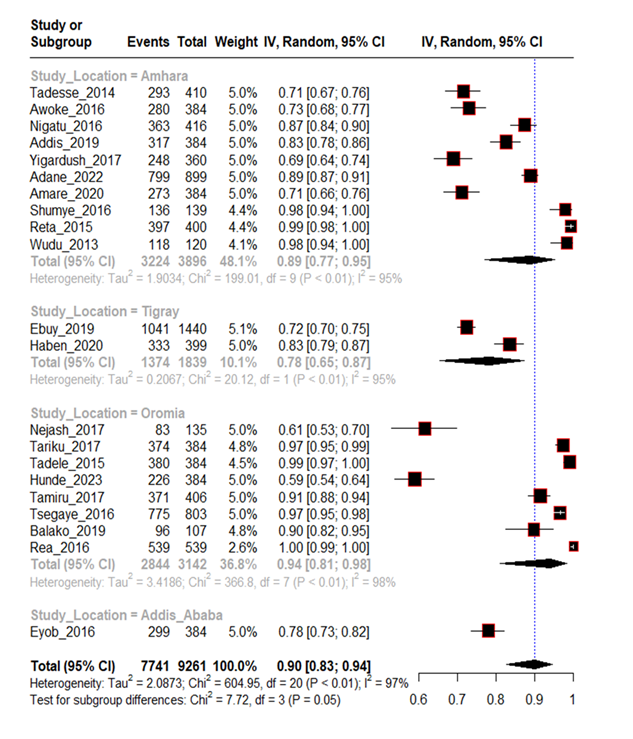
Figure 4 Sub group analysis of human rabies exposure by dogs with location
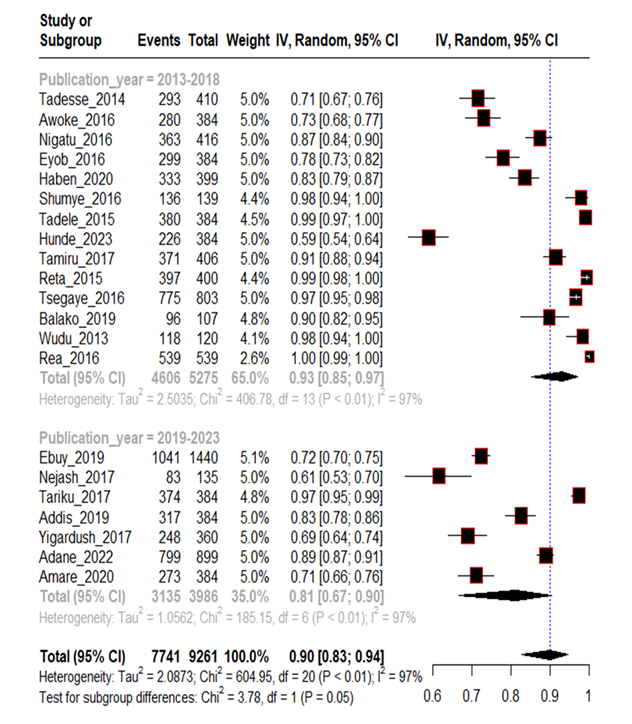
Figure 5 Subgroup analysis of human rabies exposure by dogs with publication year
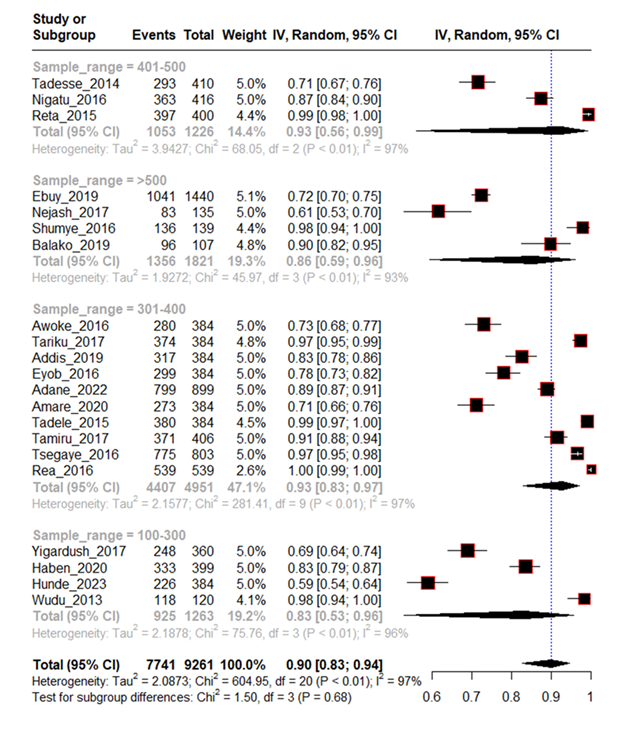
Figure 6 Sub group analysis of rabies exposure by dogs with sample size
The aim of this systematic review was to assess the pooled prevalence of dog mediated rabies exposure to humans in Ethiopia. Accordingly, the findings show a pooled prevalence of 90% (CI: 83-94, p<0.01), indicating a significant risk of dog mediated rabies in Ethiopia, with variations in regional distributions. The 7741 reports of dog-mediated human rabies exposure from 21 studies were distributed as 41.65%, 17.75%, 36.74% and 3.86% in Amhara, Oromia, Tigray and Addis Ababa respectively. The study sample sizes varied, with the smallest being 107 and the larget 1440, from studies done in Oromia and Tigray, respectively.
Majority, 66.67%, of included articles were published during the 2013-2018 period, suggesting an emerging trend of research interest in this issue. The studies reported a range of rabies exposure prevalence, from the highest of 100% to the lowest of 59%, underscoring significant regional variation and possibly differences in study methods, cultural variations, or rabies control efforts. These differences could reflect disparities in rabies control interventions, animal vaccination coverage, and public awareness campaigns across the regions. Moreover, the slight decrease in prevalence from 2013 to 2023 (from 0.93 to 0.81) indicates some progress in reducing exposure, possibly due to improved dog vaccination programs and public education.
However, the high prevalence of 90% dog mediated rabies exposure in Ethiopia remains concerning, but when compared to the global estimate of 99% for developing countries it seems better (4). The prevalence is considerably higher than a prior systematic review in Ethiopia that found a 32% prevalence of dog-mediated rabies cases (9). This discrepancy highlights the need for a nuanced understanding that rabies exposure and actual rabies cases may not always align; exposure can be mitigated through timely medical intervention, while the case fatality rate for rabies remains extremely high without post-exposure prophylaxis (PEP).
The high prevalence of dog-mediated rabies exposure underscores the need for continued and intensified efforts in rabies prevention, particularly in rural areas like Oromia and Amhara, where the burden of exposure is highest. The regional differences in rabies exposure prevalence suggest that rabies control interventions might not be equally implemented across the country. It’s essential to understand the underlying factors contributing to these disparities, whether related to geographic, economic, or healthcare access factors, and to tailor intervention strategies to the specific needs of each region. For example, areas with lower exposure rates like Addis Ababa may benefit from increased public health messaging and outreach to reduce potential hotspots, while areas like Oromia and Amhara might require more extensive dog vaccination programs
While Ethiopia has made some progress in reducing dog-mediated rabies exposure, the high prevalence remains a public health challenge. Continued focus on prevention through vaccination, education, and infrastructure development is critical. Furthermore, addressing regional disparities in rabies exposure and strengthening the healthcare response to rabies are crucial to reducing the risk of human rabies cases in the future.
This systematic review and meta-analysis has some limitations. First, included studies were heterogeneous with respect to study procedures, participants and study settings. Accordingly, our findings were summarized on a broader level, which inherently suppresses some of the unique features of different approaches. Second, the majority of studies were based on cross-sectional study design that limits the precision of prevalence of dog mediated human rabies exposure. Third, the included articles focus only on prevalence of dog mediated human rabies exposure without its determinants which makes future interventions unclear.
This systematic review highlights the significantly high (90%) risk of dog-mediated rabies exposure to humans in Ethiopia. Regional variations in exposure prevalence emphasize the need for tailored intervention strategies, especially in areas with higher prevalence like Oromia and Amhara. Despite the alarming prevalence, the slight decrease over the past decade suggests some progress in rabies control. However, continued efforts in surveillance and monitoring, dog vaccination, public education, and improved healthcare access are essential to reducing exposure and preventing rabies-related fatalities in the future.
Based on the findings of this review, authors forwarded the following recommendations:
The authors would like to acknowledge the contributions made by one health initiatives of Amhara Public Health Institute Technical Working Group.
PEP, Post-exposure prophylaxis; JBI, Joanna Briggs Institute; RNA, Ribonucleic acid; WHO, World health organization;DALYs, Disability-adjusted life years
An ethical statement is not applicable as this was merely a a systematic review and meta-analysis.
Not applicable.
All necessary information was attached to this manuscript.
The authors have no conflict of interest.
No funding was received for this project.
GDA and YKG contributed to the conception and design of the review. GDA and YKG were responsible for screening, data extraction, synthesis, and analysis of the data. GDA drafted the manuscript, which was critically revised by YKG. Rechecking together was done before the final stage of the manuscript by DS, MTM and NS.