
Scabies outbreak investigation in Shashego woreda, Southern, Ethiopia
1Public Health Emergency Management Directorate, Amhara Public Health Institute, Bahir Dar, Ethiopia
2Health Research Development Directorate, Amhara Public Health Institute, Bahir Dar, Ethiopia
3Department of Health Promotion and Health Behavior, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Ethiopia
*Corresponding Author: Eyob Mulu, Cell phone: +251918069256, Email: eyobmulu2015@gmail.com,
Background: Scabies is a contagious ectoparasite of the skin caused by the microscopic mite Sarcoptic scabies var. hominis. It is usually spread by direct and prolonged skin-to-skin contact with someone with scabies. Schools, refugee camps, and prisons are often sources of scabies outbreaks in developing countries, with the major aggravating factors being environmental (warm weather and climate change)
Objectives: To investigate and manage the outbreak, and ultimately offer recommendations for preventive measures in the Shashego district of the Hadiya zone, Southern Ethiopia, in 2018.
Methods: An unmatched community-based case-control (1:2 or 47 cases and 94 controls) nonprobability purposive sampling investigation was conducted, using predesigned questionnaires.
Results: One thousand forty-one scabies cases were reported from August to November 2018; there were no death reports. A case-control study was conducted, there were 47 scabies cases (21 males and 19 females) with a mean and median age of cases were 16 and 12 years, respectively, ranging (from 1 to 50 years) and 94 community controls (37 males and 43 females) with a mean and median age were 20.6 and 17.5 years (ranging 2-50 years). Male accounts 623(56.33%). A high attack rate of 1.69% was observed among children aged 0- 7 years. Multivariate analysis shows that infrequent use of soaps [(AOR) =15.246, 95%CI (1.901-122.268)], changing clothes once a month [(AOR)=20.668,95%CI (2.406-177.548)], washing clothes once a month [(AOR) = 66.876,95%CI (6.107-732.314)], sharing cloths with scabies case of last two month [(AOR) = 11.864,95% CI (1.664-84.562)], and prolonged direct skin to skin contact [(AOR)=54.193, CI (1.082-2714.433) were independent risk factors for scabies outbreaks.
Conclusion: The scabies outbreak occurred in the Shashego district, mainly in children 0-7 years old. Infrequent use of soaps, washing clothes once a month, changing clothes once a month, sharing clothes in families, and prolonged direct skin-to-skin contact were significant risk factors for scabies outbreaks. We recommended increasing strong active case detection and providing mass treatments. We also recommended using mass media worldwide at schools, markets, and religious places to raise awareness.
Keywords: outbreaks, risk factors, scabies, and Shashego district, Ethiopia
የጥናቱ ዳራ፡ እከክ በሳርኮፕቲክ እከክ ምክንያት የሚከሰት የቆዳ ተላላፊ ectoparasite ነው። ሆሚኒዎች. ብዙውን ጊዜ የሚዛወረው እከክ ካለበት ሰው ጋር በቀጥታ፣ ረዘም ላለ ጊዜ ከቆዳ ወደ ቆዳ በመነካካት ነው። ትምህርት ቤቶች፣ የስደተኞች ካምፖች እና እስር ቤቶች በታዳጊ አገሮች ውስጥ ዋና ዋና የአካባቢ ሁኔታዎች (የሙቀት ጊዜ እና የአየር ንብረት ለውጥ) የሚያባብሱ የእከክ ወረርሽኞች ምንጭ ናቸው። በአለም አቀፍ ደረጃ በየዓመቱ ወደ 300 ሚሊዮን የሚጠጉ የእከክ በሽታዎች ሪፖርት ይደረጋሉ። በኢትዮጵያ ውስጥ የእከክ በሽታ የተለመደ ነው፣ በቅርቡ የተከሰተውን ወረርሽኝ ካስታወስን በጥቅምት 2018 በአማራ ክልል በሚገኙ 76 ወረዳዎች ወደ 373,000 የሚጠጉ የእከክ በሽታ ተጠቂዎች ተገኝተዋል።
የጥናቱ አላማ፡ ወረርሽኙን መመርመርና መቆጣጠር እና በመጨረሻም በሻሸጎ ወረዳ ሀድያ ዞን ደቡብ ኢትዮጵያ 2018 የመከላከል እርምጃዎችን በተመለከተ ምክረ ሃሳቦችን መስጠት
የጥናቱ ዘዴ: ያልተመሳሰለ የማህበረሰብ አቀፍ የጉዳይ ቁጥጥር (1፡2 ወይም 47ኬዝ እና 94 ቁጥጥሮች) አስቀድሞ የተነደፉ መጠይቆችን በመጠቀም ያለመሆን ዓላማ ያለው ናሙና ምርመራ ተካሂዷል።
የጥናቱ ውጤት፡ ከኦገስት እስከ ህዳር 2018 በድምሩ 1041 የስካይቢስ ጉዳዮች ሪፖርት ተደርገዋል፣ የሞት ሪፖርቶች የሉም። የጉዳይ ቁጥጥር ጥናት ተካሂዶ ነበር፣ 47 የስካይቢስ ጉዳዮች (21 ወንድ እና 19 ሴቶች) አማካይ እና መካከለኛ እድሜ ያላቸው 16 እና 12 ዓመት ሲሆኑ (ከ1 እስከ 50 ዓመት) እና 94 የማህበረሰብ ቁጥጥሮች (37 ወንድ እና 43 ሴቶች) አማካይ እና መካከለኛ እድሜ ያላቸው 20.2 እና 5 አመት ናቸው። ወንድ መለያዎች 623 (56.33%)። ከ0-7 አመት እድሜ ክልል ውስጥ ያለው ከፍተኛ የጥቃት መጠን 1.69% ታይቷል። ሁለገብ ትንታኔ እንደሚያሳየው በሳሙና [(AOR) =15.246, 95%CI (1.901-122.268)] አዘውትሮ መጠቀም፣ በወር አንድ ጊዜ ልብሶችን መቀየር [(AOR)=20.668,95%CI (2.406-177.548)] በወር አንድ ጊዜ ልብስ ማጠብ (6.OR) 6፣65% 6.107-732.314)]፣ ባለፉት ሁለት ወራት ጨርቆችን ከእከክ በሽታ ጋር መጋራት [(AOR)= 11.864,95%CI(1.664-84.562)]፣ እና ረጅም ቆዳ ወደ ቆዳ ንክኪ የሚቆይ [(AOR)=54.193፣ CI(1.084-3371) ተጋላጭነት አደጋዎች ነበሩ።
የጥናቱ ማጠቃለያ፡ በሻሸጎ ወረዳ የእከክ በሽታ ተከስቷል፡ ከ0-7 አመት እድሜ ያላቸው ህጻናት በጣም የተጎዱት የእድሜ ክልል ናቸው። አዘውትሮ ሳሙና መጠቀም፣ በወር አንድ ጊዜ ልብስ ማጠብ፣ በወር አንድ ጊዜ ልብስ መቀየር፣ ልብሶችን በቤተሰብ ውስጥ መጋራት እና ለረጅም ጊዜ ከቆዳ ለቆዳ ንክኪ መቆየቱ ለስክቢያ ወረርሽኝ መከሰት አጋላጭ ምክንያቶች ነበሩ። ጠንከር ያለ ንቁ የጉዳይ ምርመራ እንዲጨምር እና የጅምላ ህክምናዎችን እንዲሰጥ እንመክራለን። በትምህርት ቤቶች፣ በገበያዎች እና በሃይማኖት ቦታዎች የመገናኛ ብዙሃንን በመጠቀም ግንዛቤን ይስጡ።
ቁልፍ ቃላት፡- ወረርሽኞች፣ የአደጋ መንስኤዎች፣ እከክ እና ሻሸጎ ወረዳ፣ ኢትዮጵያ።
Scabies is a contagious ectoparasite of the skin caused by the microscopic mite Sarcoptes scabiei var. hominis (1-3). It is usually spread by direct, prolonged skin-to-skin contact with someone with scabies(4, 5). However, it can spread easily under crowded conditions where close body and skin contact are the most common (1). Institutions in developing countries, such as schools, refugee camps, and prisons, are often sites of scabies outbreaks, with the major aggravating factors being environmental conditions (warm weather and climate change). Symptoms of scabies typically begin three to six weeks after primary infestation (4). A scabies infestation's typical signs and symptoms include superficial burrows, intense pruritus (itching), especially at night, and secondary infection. Acropustulosis, or blisters and pustules on the palms and soles of the feet, is a typical symptom of scabies in infants(6). Personal hygiene is the proper way of measuring prevention (2, 3). Scabies is a curable disease that requires topical ointment or oral administration of a scabicide agent(3, 7).
The correct number of cases of infected scabies worldwide is not known, but it is estimated to be up to 300 million annually (4). In 2001 there was a scabies outbreak in a rural Indian village where people lived overcrowded with an overall prevalence of 70%, in this year scabies outbreaks occurred among children in Australian Aboriginal communities, in Fiji, Vanuatu, and the Solomon Islands with a prevalence of 50%,18.5%, 24%, and 25%, respectively. Another scabies outbreak has occurred worldwide since 2005, in Turkey (0.4 %), Nigeria (4.7%), and Brazil (8.8%). Scabies outbreaks are common in Ethiopia. Since 2018, about 373,000 scabies cases have been reported in 76 Woredas in the Amhara region of Ethiopia (8).
However, scabies is a hygienic disease and can be prevented; the burden of scabies outbreaks is still a significant challenge in rural and urban communities and covers large geographical areas of Ethiopia. A scabies outbreak investigation conducted in the South-East Zone, Tigray Regional State, Ethiopia, 2016, shows that the scabies outbreak was a significant morbidity problem in public health (9). It is due to its nature of transmissibility, poor water access, the occurrence of the Eleno, and insufficient supply of medicines to treat those who fell ill(9). Southern Nations Nationalities and People Regional State is one of the victims of this climate change and poor water access (10). Due to this, scabies outbreaks have happened in many parts of the region, including the Shashego district and SNNPR. The scabies outbreak investigation aimed to investigate the occurrence of scabies, identify the risk factors, propose recommendations, and implement control measures that alleviate the disease burden of the community in the Shashego district.
The study was conducted in Shashego district, Hadiya zone, South Nations, Nationalities and Peoples' Regional State of Ethiopia. The district bounded by the Silte zone of SNNPR in the North, Halaba special district in the east, Kembata & Tembaro zone in the South, and the Dosha district (Hadiya zone) of SNNPR in the West, all of which were prone to scabies outbreaks. The district capital town, Bonesha, is 218 kilometers southwest of Addis Ababa, along the Addis - Arba Minch highway. Almost all parts of the district are lowland, with an annual mean temperature of about 22-240c, with the mean annual rainfall about 865-1075mm. The district’s water access was 52% (10). The district has 01 primary hospital under construction, five health centers, 36 Health posts with a total population of 132,454 (2017 to 2018 projection), and health coverage was about 81% in 2018. (Figure 1).
|
|
|
|
Figure 1 Map of Shashego district, Hadiya zone, Southern Ethiopia, 2016.
A purposive non-probability convenience sampling technique was used for case and control selection, with a case-to-control ratio 1:2. Specifically, 47 cases were identified and matched with 94 controls. Data collection involved interviews conducted using semi-structured questionnaires. Forty-seven scabies cases and 96 controls were interviewed, allowing the research team to gather comprehensive information regarding the outbreak.
Case definitions were established to ensure consistent identification of scabies cases. A suspected case was defined as exhibiting symptoms consistent with scabies, such as itching and rash. A confirmed case was determined through skin scrapings that revealed mites, mite eggs, or mite feces, as a trained healthcare professional identified. Epidemiologically linked cases were defined as suspected cases that had contact with either a laboratory-confirmed or epidemiologically confirmed case.
Data processing and analysis were done using Epi Info 7 and MS Excel. The data were checked for completeness and accuracy before entering the analysis software. Descriptive and analytical statistical methods were employed to assess the data. Logistic regression analysis was used to identify associations between scabies infection and various risk factors, with the outcome of exposure assessed through odds ratios (OR) and 95% confidence intervals (CI). Attack rates were also calculated. The results were presented through graphs, tables, and charts to understand the outbreak dynamics and associated risk factors.
Forty-seven scabies cases and 94 controls were identified from November 5, 2018, to November 16, 2018, from purposively selected two Kebeles. There was no information on scabies death (CFR=0%). The mean and median age of cases were 16 and 12 years, ranging from 1 to 50 years, and 20.6 and 17.5 mean and median age (ranging from 2 to 50 years) for controls. Of 47 cases, 26(55.3%) were males, and 51(54%) of the controls were females. The overall attack rate was 1.13%. The higher attack rate was recorded in Lay gnaw Gimbicho kebele at 1.21%, and the lower in Tachignaw Gimbicho at 1.033%. The sex-specific attack rate (SSAR) for males was 1.3% and for females, it was 0.96%.
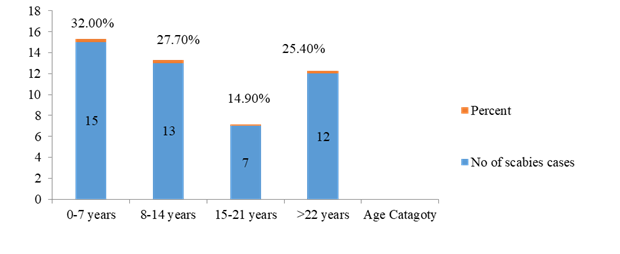
The highest cases were observed in children 0-7 years of age, 15(32%), and the least was 15-21, 7(14.9%) (Figure 2).
Figure 2 Scabies outbreak by age category, Shashego district, Hadiya zone, Southern Ethiopia, 2018.
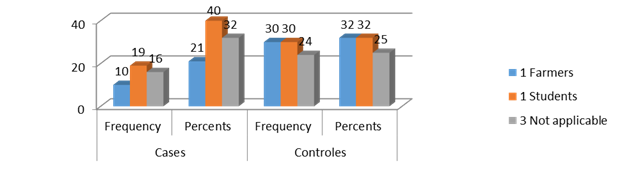
Among the total cases, about 19 (40.3%) were Muslims, and 28 (59.7%) were Protestants. 32(34%) were Muslims, 58(61%) were Protestants, and 10 (5%) were Orthodox religion followers for controls. Of the respondents, about 10(21%) cases and 30(32%) controls were farmers (Figure 3).
Figure 3 Occupation status of scabies cases and controls in Shashego district, Hadiya zone, Southern Ethiopia, 2018.
Among the total respondents, about 47% of cases and 62% of controls attended primary education (Table 1).
Table 1 Educational status of scabies cases/controls, Shashego district, Hadiya zone, Southern Ethiopia, 2018.
| Variables | Cases | Controls | ||
|---|---|---|---|---|
| Frequency | Percent | Frequency | Percent | |
| Illiterates | 12 | 25.5 | 17 | 18 |
| Primary education | 22 | 47 | 56 | 62 |
| Secondary | 0 | 0 | 2 | 2 |
| Not applicable | 13 | 27.5 | 17 | 18 |
Of 141 respondents, about 89(63.3%) know what scabies are, but three-fourths did not correctly identify the cause of scabies. Around 113(80.1%) respondents answered that personal hygiene is the prevention mechanism for scabies outbreaks. Most respondents answered correctly about scabies transmission, 122(86.5%) due to direct skin-to-skin contact and sharing clothes, and the remaining 19 due to hugging. Among the total respondents, around 114(80.9%) said they went to a health facility to seek treatment if/while they were/ were affected by scabies, and three-fourths answered scabies can be cured using modern medicine.
Among the 141 respondents, about three-fourths got 21-40 liters of water for drinking, cooking, and washing per day, while only 13 respondents got 61-80 liters of water per day (Figure 4).
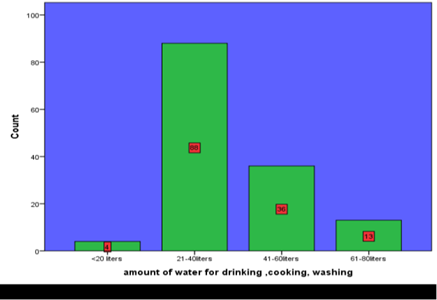
Figure 4 Daily water consumption, Shashego district, Hadiya zone, Southern Ethiopia, 2018
About 95(67.4%) of the respondents went 1-5 kilometers to Fitch water, and only a few went to 500 -1000 meters (Table 2).
Table 2 Distance to Fitch water, Shashego district, Hadiya zone, Southern Ethiopia, 2018.
| Distances | Frequency | Percent |
|---|---|---|
| 500-1000 meters | 10 | 7.1 |
| 1-5 kilometers | 95 | 67.4 |
| 5-10 kilometers | 36 | 25.5 |
| Total | 141 | 100 |
Of 141 respondents, half of the cases and controls queued for over 2 hours, only 2.84% queued for less than 30 minutes (Figure 5).
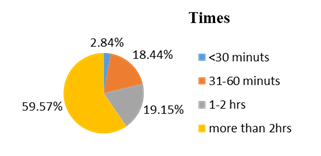
Figure 5 Queuing time for fetching water in Shashego district, Hadiya zone, Southern Ethiopia, 2018.
The trend of the outbreaks started on August 22, 2018, and continued until October 8, 2018, for almost 2 months. The index case was 18, and an 18-year-old male, Ramato Mohamed, reported on August 22, 2018, from Tachignaw Gimbicho by a health extension worker. He had a history of travel outside his home village. He had gone to Halaba special woreda to learn the Quran and came to his family one month earlier, before he had shown the signs and symptoms. Most cases were reported around September 26th and 30th, 2018 (Figure 6).
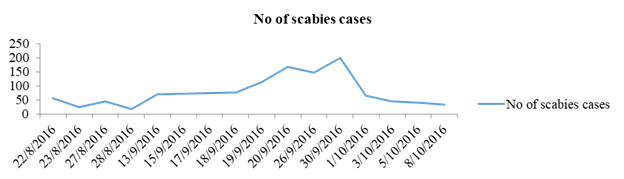
Figure 6 Scabies date of onset of itching in Shashego district, Hadiya zone, Southern Ethiopia, 2018.
Among the 47 scabies cases, 47(100%) show itching at night and a skin rash, and 20% develop a secondary infection (Table 3).
Table 3 Scabies clinical manifestation, Shashego district, Hadiya zone, Ethiopia, 2018.
| Variables | Frequency | Percent |
|---|---|---|
| Restless inching | 47 | 100 |
| Skin rash | 47 | 100 |
| Red bumps and blisters | 17 | 36 |
| Tiny red burrows | 9 | 19 |
| Crust on the skin | 20 | 43 |
| Sign of secondary infection | 4 | 8.5 |
Among the 47 cases, about 33 (70%) went to a health facility, and 27 (57%) received treatment. Among the treatment-received cases, about 22(81%) did not complete their treatments during the data collection period, and 5(19%) were re-infected after the disease was cured.
Bivariate analysis shows that prolonged direct contact with scabies cases (OR =7.217, 95%CI [2.076-25.091]), sleeping together with scabies cases (OR = 3.474, 95%CI [1.672_7.217]), and remaining in the table below were significantly associated with the occurrence of scabies (Table 4)..
Table 4 Bivariate analysis of scabies risk factors of Shashego district, Hadiya zone, southern Ethiopia, 2018.
| Independent variables | Cases | Controls | OR | 95%CL | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | yes | No | ||||||||
| N | P | N | P | N | P | N | P | Lower | Lower | ||
| Direct contact with scabies cases | 44 | 94 | 3 | 6 | 31 | 33 | 63 | 67 | 7.217 | 2.076 | 25.091 |
| Sleeping with scabies cases | 19 | 40 | 28 | 60 | 66 | 70 | 28 | 30 | 3.474 | 1.672 | 7.217 |
| Sharing cloths | 19 | 40 | 28 | 60 | 74 | 79 | 20 | 21 | 5.453 | 2.54 | 11.703 |
| Infrequent use of soaps | 9 | 19 | 38 | 81 | 38 | 40 | 56 | 60 | 2.865 | 1.243 | 6.605 |
| washing clothes once a month | 24 | 51 | 23 | 49 | 3 | 6 | 91 | 94 | 27 | 7.187 | 101.432 |
| Taking a shower once a month | 21 | 45 | 26 | 55 | 24 | 26 | 70 | 74 | 2.94 | 1.282 | 6.744 |
| Changing clothes once a month | 27 | 57 | 20 | 43 | 34 | 36 | 60 | 64 | 4.087 | 1.573 | 10.606 |
| Living in a food-insecure area | 47 | 100 | 0 | 0 | 94 | 100 | 0 | 0 | 11.846 | 4.326 | 32.436 |
| Amount of water 41-60 liters | 5 | 10.7 | 41 | 89.3 | 31 | 33 | 63 | 67 | 0.054 | 0.005 | 0.625 |
| Amount of water: 61-80 liters | 1 | 2 | 46 | 98 | 12 | 13 | 82 | 87 | 0.028 | 0.001 | 0.585 |
Multivariate analysis showed that infrequent soap use, washing clothes once a month, changing clothes once a month, sharing clothes with scabies cases, and prolonged direct skin-to-skin contact were independent risk factors for scabies outbreaks (Table 5).
Table 5 Multivariate analysis of scabies risk factors, Shashego district, Hadiya zone, southern Ethiopia, 2018
| Independent variables | cases | Controls | AOR | 95%CI | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | No | percent | No | Perce | No | percent | No | percent |
| Infrequent use of soap | 9 | 19 | 38 | 81 | 38 | 40 | 56 | 60 | 15.246 | 1.901-122.268 |
| washing clothes once a month | 24 | 51 | 23 | 49 | 3 | 6 | 91 | 94 | 66.876 | 6.107-732.314 |
| changing clothes once a month | 27 | 57 | 20 | 43 | 34 | 36 | 60 | 64 | 20.668 | 2.406-177.548 |
| Sharing cloths | 19 | 40 | 28 | 60 | 74 | 79 | 20 | 21 | 11.864 | 1.664-84.562 |
| Direct skin-to-skin contact | 44 | 97 | 3 | 6 | 31 | 33 | 63 | 67 | 54.193 | 1.082-2714.433 |
All scabies cases were registered using a scabies case-based format /line list district-wide. Routine surveillance activities were carried out and closely followed up at all levels daily. Mass treatment was given to all suspected and confirmed scabies cases with permethrin ointment and amoxicillin for those who developed secondary infection to prevent further morbidity and mortality. Health education and health information were given to the community and students at school to avoid transmitting the disease, to maximize the health-seeking behavior, and to treat the disease. At the same time, they show the signs and symptoms.
The onset of the first scabies case was the 22nd of August 2018 in Tachignaw Gimbicho kebele, as reported by a health extension worker. However, the outbreak investigation was carried out from November 5 to November 16, 2018; this is almost 2 months after, which may be due to the low awareness of the community about urgent and immediate scabicide treatment needed when there were scabies cases in the community. Of 47 cases, 26(55.3%) were males, and 51(54%) of the controls were females. The mean and median age of cases were 16 and 12 years, respectively, and ranged from 1 to 50 years, and 20.6 and 17.5 years, ranging from 2-50 years, for controls. The overall attack rate was 1.13%, the sex-specific attack rate (SSAR) for males was 1.3%, and for females, it was 0.96%. The results of this outbreak investigation provide useful findings regarding risk factors for scabies outbreaks in the study population. Both of the two kebeles had low water access for personal hygiene.
Therefore, the results are still helpful in the context of the study. Our study indicates that there is a significant burden of scabies disease in children between the ages of 0 and 7 years. The finding may be truly expressed; this age group does not maintain good hygiene, and mostly spends their time playing with mud/soil. Nearly half of the scabies cases were reported among students; it may be true that students have had contact with scabies-infested persons, and schools are also a source of scabies infestation. Although the sample size was not calculated precisely, keeping in mind the disease frequency, cases that fulfilled the inclusion criteria during the study period in purposely selected kebeles were included.
The potential risk factors included in our investigation were infrequent use of soaps, washing clothes once a month, changing clothes once a month, sharing clothes with scabies cases, and prolonged direct skin-to-skin contact. Sharing clothes with a person with scabies infestation was found in our study to be one of the risk factors contributing to the occurrence of scabies. Individuals who share clothes were 20.668 times more prone to having scabies than those who do not share clothes. The reason is probably that poor socioeconomic status makes it difficult to buy clothes, or it may be due to low awareness of scabies transmission by sharing clothes. A retrospective survey conducted in Portugal shows that poor socio-economic status and low awareness of the transmission of scabies through sharing clothes were associated with scabies (1). The prevalence of scabies was 18.5% among primary school children and 14.0% in infants (11). Personal hygiene practices seem important in acquiring scabies; poor hygienic practices are associated with higher rates of family infestation (12). Changing clothes once a month was a significant risk factor in this study. It has often been suggested that fertilized female S. scabies mites are responsible for scabies transmission. Still, their relatively small number and inclination to remain within burrows make it seem unlikely. A greater number of immature mites on the skin surface appears necessary to transmit the disease (12, 13). It is quite possible that frequent use of soap for personal hygiene removes immature mites from the skin, and the number of these mites would be reduced, which would reduce the probability of scabies transmission (14).
In our study, infrequent use of soap for personal hygiene was a significant risk factor for scabies. The spread of scabies through infested clothes, prolonged direct skin-to-skin contact, and sleeping together were the main risk factors for the spread of scabies (13, 14). Scabies mites live their entire lives on human skin as obligate parasites, and can only live outside the human body for up to 48 hours, making transmission through skin contact possible (15). Our study found that sharing clothes and prolonged direct skin-to-skin contact were the risk factors for scabies outbreaks, but sleeping together was unlikely.
A scabies outbreak occurred in the Shashego district; children aged 0-7 were the most affected age group. Infrequent use of soaps, washing clothes once a month, changing clothes once a month, sharing clothes in families, and prolonged direct skin-to-skin contact were significant risk factors for scabies outbreaks. We recommended increasing strong active case detection and providing mass treatments. We also recommended using mass media worldwide at schools, markets, and religious places to raise awareness.
We thank Hawassa University, College of Health Sciences, School of Public and Environmental Health, for approving ethical clearance for data collectors, supervisors, and study participants.
SNNPRS South Nation, Nationality, People, Regional State
MM Millis Meters
WHO World Health Organization
SPSS Software package for social science
Epi Epidemiological information
OR Odd Ratio
CI Confidence interval
CFR Case Fatality Rate
SSAR Sex specific Attack Rate
AOR Adjusted Odds Ratio
SNNPRS South Nation, Nationality, People, Regional State
Ethical approval was obtained from the Institutional Review Board of Hawassa University, College of Medicine and Health Science. After a clear explanation about the study's aim and the privacy of the data, consent was obtained from the mothers/caretakers of the children. Strict measures were taken to maintain the confidentiality of the information throughout the study.
Not applicable.
Data will be available upon reasonable request from the corresponding author.
The authors declare that they have no competing interests.
No funding was obtained for this study.
EM designed the study, participated in data collection, analyzed and interpreted data, drafted the paper, and revised the manuscript. AN assisted with the design, took part in drafting the article or revising it critically for important intellectual content, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.