Dietary Diversity Practices and Nutritional Status among Children Age 6-59 Months in Armed Conflict Affected Areas of Amhara Region, Ethiopia.
Hailu Ayalew Adgeh1*, Netsanet Fentahun2, Betelehem Belete Akine1, Abraham Amsalu1, Belay Bezabih1, Mulat Tirfie2, Yosef Beyene, 3 and Girum Meseret Ayenew 1
1Amhara Regional State Public Health Institute
2 Bahir Dar University
3 Ethiopian Public Health Institute
*Corresponding Author: Hailu Ayalew Adgeh email; hailuayalew07@gmail.com, mobile; 0946292071
Background: Appropriate and adequate feeding practice is a pre-requisite to good nutritional status in any given time of human life. Globally, around 136 million people needed assistance due to armed conflict, while more than 52 million children suffer from acute malnutrition. Armed conflict triggers food insecurity and affects child nutrition through disrupting crop production, destroying food stores and livestock, forcing people to eat foods with lower nutritional value, affecting market food supply and price inflation. This study aimed to determine dietary diversity practice and nutrition status of children age 6-59 months in the armed conflict affected areas of Amhara region, Ethiopia.
Methods: Community based Cross sectional study design was employed among children age 6-59 months in armed conflict affected areas of Amhara region from March 13, 2022-April 13, 2022. A Multi-stage cluster sampling procedure was used to select households. The total sample size was 2571 children of age 6-59 months. Data was collected using interviewer administered questionnaire adapted from Food and Nutrition Technical Assistance and food and agriculture organization. A 24-h recall method was used to assess dietary diversity practices of children. Anthropometric measurements were done to get height and weight of children. The collected data using Open Data Kit was extracted from the server to excel version 2016 and were cleaned and coded for further analysis using SPSS version 25.
Result: About 2582 children were included in the present study. The prevalence of adequate dietary diversity practice was 7.6 % in the study area. The food groups eaten by most (90.9%) of the children in the past 24 hours were grains, roots and tubers whereas the least (1.9%) food groups were flesh foods. The study showed that 13.6%, 27.7% and 41.6% children were wasted, underweight and stunted respectively. About 5.3%, 8.9% and 21.1% of them were severely wasted, underweighted and stunted respectively. About 2.3% of index children had illness in the past two weeks.
Conclusion and recommendation: the level of adequate dietary diversity practice for children age 6-59 month in the study area was very low. The level of acute malnutrition, underweight and stunting in the study areas were very high. This evidence indicates the urgent need of providing emergency nutrition service to manage children with acute malnutrition. Micronutrient supplements should be given for children in regular pattern.
Keywords: Dietary diversity practice, child nutritional status, armed conflict, Amhara region
የጥናቱ ዳራ፡ ተገቢነት ያለውና በቂ የአመጋገብ ተግባር በማነኛውም የሰው ልጅ ህይዎት ውስጥ ለተሻለ የስርዓተ ምግብ ይዘት እንደቅድመ ሁኔታ የሚወሰድ ተግባር ነው። በአለም አቀፍ ደረጃ ወደ 136 ሚሊዮን የሚሆን ህዝብ በጦርነትና በግጭት ምክንያት አስቸኳይ ድጋፍ የሚያስፈልጋቸው ሲሆን ከ52 ሚሊዮን በላይ የሚሆኑ እድሜአቸው ከ5 ዓመት በታች የሚሆኑ ህጻናት በአጣዳፊ የምግብ እጥረት እይተሰቃዩ ይገኛሉ። በታጠቁ ሀይሎች መካከል የሚደረግ ግጭት የሰብል ማምረት ሄደትን በማደናቀፍ፥ የምግብ ክምችትንና እንስሳትን በማውደም፥ ሰዎችን ዝቅተኛ ጠቀሜታ ያለችውን ምግቦች እንዲመገቡ በማስገደድ፥ በገበያ ላይ የምግብ እህሎች አቅርቦትን በመቀነስና የምግብ ዋጋን በመጨመር የምግብ ዋስትና ያሳጣል፤ ለምግብ አቅርቦት እጥረትም ይዳርጋል።
የጥናቱ ዓላማ፡ ይህ ጥናት በአማራ ክልል ውስጥ በሚገኙ በጦርነት ጉዳት በደረሰባቸው አካባቢዎች የሚኖሩ እድሜአቸው ከ6-59 ወር ያሉ ህጻናትን የተለያዩ የምግብ ዓይነቶቸን የመመገብ ትግበራ /ልምድ/ና የእነዚህን ህጻናት የአመጋገብ ሁኔታን ለመወሰን የተካሄደ ጥናት ነው።
የጥናቱ ስልቶች፡ ለዚህ ጥናት ማህበረሰብ አቀፍ የጥናት ንድፈ ወይም ዘዴና የአንድ ጊዜ የመረጃ ስብሰባን የተጠቀምን ሲሆን ጥናቱ የተካሄደው በጦርነት ጉዳት በደረሰባቸው የአማራ ክልል አካባቢዎች ውስጥ በሚኖሩ እድሜአቸው ከ6-59 ወር በሆኑ ህጻናት ላይ ነው።መረጃውን ከመጋቢት 4/ 2014 እስከ ሚያዚያ 5/2014 ዓ.ም የሰበሰብን ሲሆን የጥናቱ ተሳታፊዎችን ለመምረጥ ብዙ ደረጃዎችን በጎራ በመክፈል / መልቲ ሌቭል ክላሰተር/ የጥናት ተሳታፊዎችን ለመምረጥ ይህን ዘዴ ተጥቅመናል። በጥናቱ በአጠቃላይ እድሜአቸው ከ6-59 ወር የሆኑ 2571 ህጻናት ይካተታሉ ተብሎ ተወስኗል። መረጃውን ለመሰብሰብ ከፋንታ ፕሮጀክትና ከአለም የምግብና የግብርና ድርጅት የተወሰዱ መጠየቆችን በመጠቀም የመረጃ ሰብሳቢዎች ለህጻናት ወላጆች ወይም ተንከባካቢዎች በቀጥታ ባቀረቡት ጥያቄ መሰረት መረጃው ተሰብስቧል። ህጻናትን የተለያዩ ምግቦችን የመመገብ ትግበራን/ልምድን/ ለማወቅ ወላጆች ወይም ተንከባካቢዎች በባለፈው 24 ስዓት ውስጥ በመጠየቁ ለተካተቱት ህጻናት ምን ምን የምግብ አይነቶች እንደሰጧቸው በመጠየቅ መረጃው ተሰበስቧል። በጥናቱ የተካተቱ ህጻናትን ቁመትና ክብደት ለማግኘት የልጆች የሰውነት ልኬታ ተሰርቷል። በኦዲኬ የተሰበሰበው መረጃ በኤክስ ኤል 2016 ከጸዳና መለያ ኮድ ከተሰጠው በኋላ በኤስ ፒ ኤስ ኤስ 25 በመተንተን የጥናቱን ግኝቶች ለማውጣት ተስርቷል።
የጥናቱ ውጤት፡ በጥናቱ በአጠቃላይ 2582 ህጻናት ተካተዋል። በጥናቱ በተካተቱ አካባቢዎች ተገቢ የሆነ ህጻናትን የተለያዩ ምግቦችን የመመገብ ትግበራ ምጥነት 7.6% መሆኑን ጥናቱ አሳይቷል። መረጃው ከመሰበሰቡ ከ24 ስዓት በፊት በነበረው ጊዜ ውስጥ በአብዛኞቹ (90̈.9%) የጥናቱ ተሳታፊዎች ህጻናት ለምግብነት የዋሉ የምግብ ክፍሎች የእህል ዘሮች፥ ስራስሮችና የአገዳ እህሎች ሲሆኑ በጣም በጥቂቶች(1.9%) በሚሆኑት ተሳታፊዎች ለምግብነት የዋሉት ስጋና የስጋ ተዋጽኦች ናቸው። ጥናቱ 13.6% ፣ 27.7% እና 41.6% የሚሆኑት ህጻናት እንደየቅደም ተከተላቸው የቀጨጩ፥ ዝቅተኛ የሰውነት ክብደት ያላቸውና እና የቀነጨሩ መሆናቸወን አሳይቷል። ከእነዚህም ውስጥ 5.3%፣ 8̈.9% እና 21.1% የሚሆኑት እንደየቅደም ተከተላቸው በጣም የቀጨጩ፥ በጣም ዝቅተኛ የሰውነት ክብደት ያላቸውና፥ በጣም የቀነጨሩ ነበሩ።
ማጠቃለያዎችና ምክረ ሃሳቦች፡ በጥናቱ በተካተቱ አካባቢዎች ከ6-59 ወር እድሜ ላላቸው ህጻናት ተገቢ የሆነ የተለያዩ ምግቦችን የመመገብ ትግበራ በጣም ዝቅተኛ ነበር። በጥናቱ በተካተቱ አካባቢዎች የአጠዳፊ የምግብ እጥረት ወይም መቀንጨር፥ዝቅተኛ የሰውነት ክብደትና የመቀንጭር ምጣኔ በጣም ከፍተኛ ነበር። ህጻናትን የተለያዩ የምግብ አይነቶችን የመመገብ ትግበራን ለማሻሻል በጦርነቱ ለተጎዱ አካባቢዎች አስቸኳይ የምግብ ድጋፍ ማድርግ፣ በአጣዳፊ የምግብ እጥረት የተጠቁ ህጻናትን ለማገዝ አስቸኳይ የድንገተኛ የስርዓት ምግብ አገልገሎት መስጠትን እና ለህጻናት ሰውነት በጥቂት የሚፈለጉ የምግብ አይነቶችና ንጥረ ነገሮች እድላ ማድረግን እንመክራለን።
የጥናቱ ቁልፍ ቃላት፡ የምግቦች ስብጥር ትግበራ፤ የህጻናት የስርዓተ ምግብ ሁኔታ፤ የታጠቁ ሀይሎች ግጭት፤አማራ ክልል
Globally, malnutrition is one of the most serious public health concerns. It affects the publics social and economic development in different ways. It contributes directly or indirectly for the death of 45% of the 5.9 million under-five children in 2015.1,2 This is the reason why adequate nutrition is identified as one of the pillars of public health interventions worldwide. 3
Appropriate and adequate feeding practice is a pre-requisite to good nutritional status in any given time of human life because consumption of nutritionally inadequate diet can lead to poor nutritional status.4
The most common cause of malnutrition at the individual level is inadequate dietary diversity that does not provide adequate calories and micronutrients.1,5 Micronutrient deficiency is caused by chronic deficiency of vitamins and minerals as a consequence of nutrient inadequacy.2,3,6,7 Dietary assessment is conducted to measure the nutritional adequacy of an individual’s food that provides information about the types and quality of foods consumed in terms of nutrient adequacy and also consumption patterns and behaviors of the people.8 It is the quantification of the number of different foods or food groups consumed over 24-hour period.9 The dietary diversity score has been identified as a potentially useful indicator of nutrient adequacy of children’s diets.10,11,12 This score can be used to assess the macro and micronutrient consumption levels.13, 14 The World Health Organization (WHO) recommends that children should consume at least four foods from the seven food groups.11
Majority of the world’s children who have acute and chronic malnutrition are found in South Asia and sub-Saharan Africa than elsewhere in the world.12 In African, more than 200 million under-fives years’ children suffered from malnutrition and failed to reach their full cognitive potential. In Ethiopia, both acute and chronic malnutrition are the major public health problems. The prevalence of acute malnutrition in Ethiopia was 10% and the prevalence of stunting in under-five children was 37%.15
Humanitarian crises have affected millions of people, which exacerbate nutritional risks and often lead to acute malnutrition. Globally, around 136 million people need assistance due to armed conflict, while more than 52 million children suffer from acute malnutrition.16 Developing countries face triple burden of malnutrition. This is more complicated where there is an increase in conflict, population displacement and urban warfare. During armed conflict, food and nutrition insecurity becomes increasingly worse in conflict affected areas.17
Conflicts are bound to affect the food and nutrition situation of the local population in a variety of ways. Productive activities are disrupted, food stores are looted or destroyed, livestock is slaughtered, insecurity and landmines prevent people from growing crops, people hiding in the forests are obliged to feed on wild foods, host families share their resources with displaced relatives or orphans, market supply and prices are affected, and all of the above undermine household food security and nutritional status. 18
In recent times, conflict has been identified as a key driver, accounting for the increase in global food insecurity from 777 million in 2015 to 815 million in 2016. 19 Some of the countries plagued by conflict in the recent decades are characterized by widespread hunger and chronic undernutrition. More recent evidence found armed conflict as a significant predictor of acute malnutrition and food insecurity in Africa especially in Ethiopia. 20
Armed conflict triggers food insecurity and affects nutrition through disrupting crop production, destroying food stores and livestock, forcing people to eat food with lower nutritional value, affecting market food supply and price inflation; pushing people to live in unhealthy environments; impacting health services; and affecting productivity and family care structures. 21
Undernutrition due to inappropriate-feeding practice is an important public health problem in Ethiopia; especially, in Amhara region where much of the people were living in worse condition due to the conflict. However; there is no adequate study that showed the impact of armed conflict on child dietary diversity and nutritional status in Amhara region. This study therefore aimed to determine dietary diversity practice and nutrition status of children age 6-59 months in the armed conflict affected areas of Amhara region, Ethiopia.
The study was conducted in armed conflict affected areas of Amhara region from March 13, 2022-April 13, 2022. The study sites were North Wollo, South Wollo, North Gondar and Wag Himra zones.
Based on the 2007 Census conducted by the Ethiopia central statistical Agency, North wollo zone has a total population of 1,506,498. In this zone, subsistence agriculture is the main livelihood of the rural population. Climatic condition of the zone is 23.3% Dega, 47.2% woyna Dega and 29.5% kola. the major crops produced are teff, barley, sorghum, wheat, peas and beans.22 ccording to the 2007 Ethiopian Census, there are 569 637 people living in the Wag Himra zone. Subsistence farming provides the majority of the rural community's income. The zone's main agricultural products include millet, barley, sorghum, wheat, teff, beans, peas, and honey.23,24 based on the Ethiopia 2007 Census, North Gondar zone has a total population of 948,170. Climatic condition of the zone is 16% Dega, 30% woyna Dega 44% kola and wurch 10%. The major crops cultivated in the zone are, millet, barley, sorghum, wheat, teff and sesam. 25
Community based cross sectional study design was employed in armed conflict affected areas of Amhara region.
The study population were all children age of 6-59 months living in selected armed conflict affected zones and woredas of Amhara region. All children age 6–59 months old in the study areas irrespective of ethnicity, religion and sex, were included in the study. All Children 6–59 months of age and their mothers who did not live for at least 6 months in study area were not included in the study.
The sample size was calculated by using single population proportion formula with previous prevalence of 15%.26 design effect 2, 95% CI, 2% precision and 5% non-response rate.
The total sample size was 2571 children of age 6-59 months.
A multi-stage cluster sampling procedure was used to select households. Four war affected zones were selected purposively. Fourteen woredas from these affected zones were allocated proportionally by simple random sampling technique (four woredas from each zones of Wag Himra and North wollo and three woredas from each zones of North Gondar and South wollo were included). Three kebeles from each selected woredas were included by simple random sampling technique. Then the selected kebeles were clustered by villages and one got or village was taken as cluster and all the targets in the cluster were taken as study units.
Data was collected using interviewer administered questionnaire and anthropometric measurements. The questionnaire adapted from FAO,27 FANTA28 and WHO8 was prepared in English and then translated into local language Amharic. It was loaded to the open data kit (ODK) system to collect data electronically. After the recruitment process of data collectors and supervisors, training on data collection tools, interview techniques and application of ODK with pretest was given.
A 24-h recall method (from sun rise to sun rise) was used to assess dietary diversity practices of children. The data was collected based on the mother’s/care giver’s recall of foods given to her child in the previous 24 hours prior to the interview date. The dietary diversity practice was assessed using the information collected from the 24-hour dietary recall. Dietary diversity was classified as either adequate or inadequate. Dietary diversity was taken as adequate if a child had received four or more food groups from the eight WHO food groups in the past 24 hours preceding the survey date. The eight food groups included were, breast feeding; grains, roots, and tubers; legumes and nuts; dairy products (milk, yogurt, and cheese); flesh foods (meat, fish, poultry, and liver/organ meats); eggs; vitamin rich fruits and vegetables; and other fruits and vegetables.28
Children’s height and weight were measured. Body weight was measured using portable weighing scale in light clothing with no jackets or coats, shoes, and additional clothing to the nearest 0.1 kg. For child less than two or unable to stand the difference between weight of the mother caring the child and the weight of the mother alone on a new calibrated portable scale was taken. Weighing scale was calibrated before and after any measurement.
Height of children was measured using a portable studio meter with no shoes; the shoulders, buttocks, and the heels touched the vertical stand with the head in Frank fort’s position to the nearest 0.1cm. Children with 6-23 months of age, recumbent length the nearest to 1mm and for children 24-59 months of age, standing height to the nearest 0.1 cm will measure.
All anthropometric measurements were taken twice, and the average of the two measurements was calculated and recorded. For children under-5 years of age, the presence of nutritional edema was also assessed. The edema assessment was used in the classification of the children ‘s nutritional status.
To assure the quality of the study, different precautions were taken prior to data collection, during data collection, data entry and analysis. Training was given and pretest was done. At the end of each data collection date, the server data come from ODK was extracted and examined for its completeness and consistency by the investigators and pertinent feedbacks had been given to the data collectors and supervisors to correct.
Dietary diversity practice and nutritional status; wasting (weight for height), stunting (height for age) and underweight (weight for age) of children were used as the dependent variable.
Child age, sex, and number of under five children, Maternal age, marital status, occupation, educational level, residence, and family size, partner educational status, occupation and other sociodemographic characteristics were taken as independent variables.
Descriptive analysis approaches were used to address the stated objectives. The collected data using ODK was extracted from the server to excel version 2016, cleaned and coded for analysis using SPSS version 25. Descriptive statistics like frequency, percentage and mean were carried out for different variables. Children’s age, sex, height and weight were entered into WHO Anthro Plus 2007 software to generate indices of weight-for-age, weight-for-height and height- for- age. The indices were converted into Z-scores by taking age and sex of children into consideration. Those children who have Z score below -2 standard deviations of the WHO median reference for weight-for age (WAZ), weight-for-height (WHZ) and height-for age (HAZ) were defined as underweight, wasted, and stunted respectively. The descriptive part of the result was presented using text, tables and figures.
Armed conflict: mean devastating loss of civilian life, massive displacement and violations of human rights and international humanitarian law.29
Affected areas: these were the areas in Amhara region where the armed conflict was conducted.
Stunting (HAZ): is a form of under nutrition defined as low height-for-age (when the height for age is <-2 Z score)
Underweight: Underweight is a composite form of undernutrition, including elements of stunting and wasting, and is defined by a Weight-for-Age z-score below -2.
Acute malnutrition (WFH): Acute Malnutrition is a form of undernutrition defined by the presence of bilateral pitting edema or wasting – a low Mid-Upper Arm Circumference (<12.5cm) or a low Weight-For-Height (<-2 Z Score).
Adequate dietary diversity practice: it is the practice of child feeding when 4 or more food groups eaten by children from 8 food groups within the past 24 hours irrespective of the quantity
Inadequate dietary diversity practice: it is practice of child feeding when < 4 food groups eaten by children from 8 food groups within the past 24 hours irrespective of the quantity
A total of 2582 children age 6-59 months with the response rate of 100% were included in the survey. The male-to-female ratio was 1.004. The mean (±SD) age of children was 27.6 (±13.82) months. The mean age of mothers was 30 (±6.32) years. The mean family size of the households was 5 members with SD (±1.71). (Table 1).
Table 1. Socio demographic characteristics of the study subjects in armed conflict affected zones, Amhara region, North West Ethiopia, 2022
| Variable | Category | Frequency | Percentage |
|---|---|---|---|
| Age of the child | 11-Jun | 333 | 12.9 |
| 23-Dec | 724 | 28 | |
| 24-35 | 638 | 24.7 | |
| 36-47 | 490 | 19 | |
| 48-59 | 397 | 15.4 | |
| Family size | < 3 | 676 | 26.2 |
| 6-Apr | 1494 | 57.9 | |
| >7 | 412 | 16 | |
| Maternal age | 16-23 | 565 | 21.9 |
| 25-34 | 1396 | 54.1 | |
| 35-44 | 542 | 21 | |
| 45-49 | 79 | 3.1 | |
| Sex of child | F | 1293 | 50.1 |
| M | 1289 | 49.9 | |
| Water access | <=30 min | 1256 | 48.6 |
| 31-60 min | 723 | 28 | |
| >60min | 572 | 22.2 | |
| Partner occupational status | 319 | 12.4 | |
| Daily laborer | 212 | 8.2 | |
| Employed | 262 | 10.1 | |
| Farmer | 1530 | 59.3 | |
| House wife | 12 | 0.5 | |
| Merchant | 168 | 6.5 | |
| Others | 69 | 2.7 | |
| Student | 10 | 0.4 | |
| Partner educational level | 320 | 12.4 | |
| Unable to read and write | 910 | 35.2 | |
| Able to read and write | 347 | 13.4 | |
| Primary | 549 | 21.3 | |
| Secondary | 285 | 11 | |
| University | 171 | 6.6 | |
| Maternal educational status | Unable to read and write | 1331 | 51.5 |
| Able to read and write | 179 | 6.9 | |
| Primary school | 634 | 24.6 | |
| Secondary school | 294 | 11.4 | |
| University | 144 | 5.6 | |
| Marital status of the respondent/ care giver/ | Divorced | 218 | 8.4 |
| Married | 2259 | 87.5 | |
| Single | 56 | 2.2 | |
| Widowed | 49 | 1.9 | |
| Occupation | Daily laborer | 128 | 5 |
| Employed | 123 | 4.8 | |
| Farmer | 1040 | 40.3 | |
| House wife | 1035 | 40.1 | |
| Merchant | 199 | 7.7 | |
| Others | 35 | 1.4 | |
| Student | 22 | 0.9 | |
| Residence (Address) of the care giver/ mother | Rural | 2097 | 81.2 |
| Urban | 485 | 18.8 | |
| Water access | <= 30 min | 1256 | 49.20% |
| >30 min | 723 | 28.30% | |
| >60 min | 572 | 22.40% |
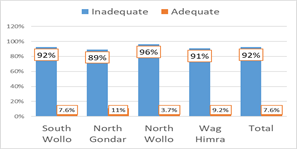
Among all children of 6-59 months old, the finding showed that only 7.6 % of the participants had adequate dietary diversity practice. The prevalence of adequate dietary diversity practice among children aged 6-24 months was only 7.2%. Adequate dietary diversity practice was very low (3.7%) in North Wollo zone and relatively higher in North Gondar (11%). It was also lowest among children who have single (7.6%) and divorced (5%) mothers than married mothers (8%). It was also low among children whose mothers/caregivers did not have formal education (7.1%) than children whose mothers’ /care givers have educated to university level (16%). Children whose mothers were daily laborer (5.5%) and housewife (5.7%) have the highest Dietary diversity than other than other occupations (Figure 1).
Figure 1. Dietary diversity practice in armed conflict affected areas of Amhara region, Northwest Ethiopia ,2022
Adequate dietary diversity practice among males & females was almost similar (M= 7.7% & F7.5%). The finding showed that relatively adequate dietary diversity practice was better in urban areas (9.5%) than rural areas (7.5%). It was relatively better among children age 12-23 months (8.6%) than other age groups (Figure 2).
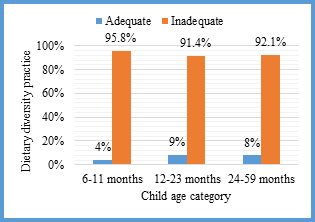
Figure 2. Child Dietary diversity practice by age category in armed conflict affected areas of Amhara region, Northwest Ethiopia, 2022.
Breast feeding is common in Ethiopia and 95.5% of children age 6-11 months and 60.6% of children age 6-23 months were on breast feeding in the study area. The food groups eaten by most (90.9%) of the children in the past 24 hours before the interview day were grains, roots, and tubers whereas the least (1.9%) food groups eaten by children were flesh foods (Figure 3).
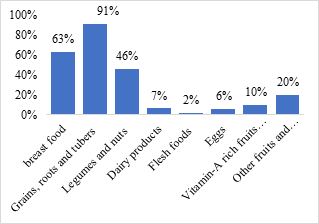
Figure 3. Food consumption by children in the past 24 hours before the interview day in armed conflict affected areas of Amhara region, Northwest Ethiopia,2022.
The current study showed that 13.6%, 27.7 and 41.6% of children age 6-59 months were wasted, underweight and stunted respectively. About 5.3%, 8.9% and 21.1% of them were severely wasted, underweighted and stunted respectively. The magnitude of acute malnutrition was higher in Wag Himra (24.1%) and smaller in south Wollo zone (7.2%).
The magnitude of acute malnutrition in the current study was higher among urban residents (19.1%) than rural (12.4%). It is also higher among households which have three or more under five children than households that have one under five child. It is higher among children whose mothers were single (20.8%), widowed (16.3%) than married (13.3%) (Figure 4).
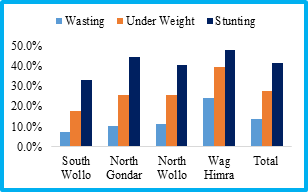
Figure 4. The nutritional status of children age 6-59 months in armed conflict affected areas of Amhara region, North West Ethiiopia,2022.
The nutritional status of children can be affected by illness and health care services available in the area. The result showed there were currently sick family members in 310 (12%) of participants’ households. The common symptoms of illness for these family members were cough (37.4%), fever (45.8%), Diarrhoea (22.3%) and fatigue (11%).
The result also showed that 59 (2.3%) of the index children had had illness in the past two weeks before the data collection date. The most common signs of illness were cough (45.8%), fever (66.1%), diarrhoea without blood (15.3%), and diarrhoea with blood (10.2%). Among these children, only 35 (59%) of the mothers sought medical help for the current illness of the child. Seventeen percent (17%) of the index children slept under the bed net in the last night.
About half (49.2%), 28.3% and22.4% of the household’s access water within 30 minutes, 30-60 minute & > one hour including waiting time respectively. The most common source of drinking water was public tap (42%) followed by protected hand dug well (18%) and pipe water (16.2%). For the rest the most common water source was from unprotected sources (river, unprotected spring, unprotected well). About 88.5% and 54.3% of the participants have hand washing practice before eating and before feeding their child respectively.
Dietary diversity scores have been validated for several age/sex groups as proxy measures for macro and/ or micronutrient adequacy of the diet.30 Dietary diversity practice scores have been positively correlated with adequate micronutrient density of complementary foods for infants and young children, and macronutrient and micronutrient adequacy of the diet for non-breast-fed children.28 In this study we measured the dietary diversity practice of children age 6 to 59 months in war affected areas of Amhara region. The overall magnitude of adequate dietary diversity practice was 7.6% and for children 6-23 months was 7.2% which was smaller than finding of EDHS 201631 and the study done in South Ethiopia-Gedeo zone.28 South Tigray, 32 North-Central Ethiopia, 33 and Madagascar.34 This might be due to the impact of the war that affected the food and nutrition security of the conflict affected areas.
Children whose mother’s/care givers had no formal education had low (7.1%) dietary diversity practice than those whose mothers’/care givers had educated to secondary school (10.2%) and university level (16%). The possible reason might be educated mothers/ care givers might have information and awareness about child feeding including dietary diversity practice. Similar findings were reported from Kenya,26 Madagascar,34 south Tigray, 32 South Ethiopia.35 Dietary diversity practice was also lowest among children whose mothers were single (7.6%) and divorced (5%) than married mothers (8%). This might be because of single and divorced mothers might have economic shortage to feed diversified food to their children. Children whose mothers were daily laborer (5.5%) and house wife (5.7%) have the lowest Dietary diversity practice than employed mothers. The possible reason may be employed mothers might have better information and knowledge about child feeding and household management with their monthly salary.
Children age 12–23 months had better dietary diversity practice than children age 6-11 months. This might be due to mother’s attitude and practice during 6–11 months who might not introduce diversified foods; they might focus on breast feeding and simply introduce fewer foods in the form of liquid or semi solid foods. The finding is similar to the findings reported from EDHS 2016.31
The prevalence of global acute malnutrition /wasting/ in the current study was 13.6 % with 5.3% of sever wasting. It is higher in males (7.3%) than females (6.3%). The prevalence is also higher in rural areas (10.1%) than urban areas (3.6%) in the study area. It was higher among children age 6-11 months (19.4%) than all other age groups. This might be due to inadequate and inappropriate complementary feeding practice. It was also higher among children which have high family member (15.3%) than households with low family members. The possible reason might be mothers who have high number of family size may have economic shortage. Wasting was highest among children whose mothers were single (20.8%) and widowed (16.3%) than married (13.3%). The reason might be single and divorced women might have no food and nutrition security because of economic shortage.
The prevalence of acute malnutrition was lower than the finding reported in Ethiopian Somali36 and the finding reported in a systematic review of Ethiopia.26 The prevalence was higher than the prevalence reported in the finding of EDHS 201631 & Mini EDHS 2019.37 It is also higher than the finding reported in Cameron,38 North west Ethiopia -Zege39 South Ethiopia-Damot Gale,35 Lalibela town.40 This difference might be due to the household’s food and nutrition insecurity that resulted from the impact of the conflict.
The prevalence of under-weight (weight for age) in the current survey was 27.7% which was congruent to the prevalence reported in Cameron38 & south Ethiopia.35 It was higher than the prevalence reported in Ethiopian Somali36 & Lalibela town.40 It was also higher than the national prevalence reported in mini DHS 2019.37
The prevalence of stunting in this survey was 41.6% which was aligned with the finding reported in a systematic review in Ethiopia.26 It was higher than the finding in North East Ethiopia,41 EDHS 2016.31 It was almost similar to the regional prevalence of stunting reported in mini EDHS 201937 but lower than the regional prevalence reported in EDHS 2016 (46.3%).31 This showed the immediate consequence of the conflict which contributed to high level of household food insecurity and inadequate dietary diversity that ends with acute malnutrition.
The prevalence of adequate dietary diversity practice among children in the study areas was very low. The prevalence of acute malnutrition under-weight and stunting were very high in the study area as compared to other studies in the country.
We recommend urgent food support to the war affected areas to improve dietary diversity of children. This evidence indicates the urgent need of providing emergency nutrition service to manage children with acute malnutrition. Micronutrient supplements should be given for children in regular pattern to improve the nutritional quality.
DHS: Demographic and Health Survey Report,
FANTA: Food and Nutrition Technical Assistance,
FAO: food and agriculture organization,
AZ: height-for age,
ODK: Open Data Kit,
SD: standard deviation,
AZ: weight-for age,
WHZ: weight-for-height,
WHO: World Health Organization.
Ethical approval was obtained from Institutional Review Board (IRB) of the Amhara national regional state Public Health Institute (APHI) before the study. Participation in the study was on a voluntary basis. Privacy and confidentiality were maintained. Sick and severely malnourished children were advised and referred to the nearest health facilities and nutritional advice was given to mothers.
All the datasets analyzed during the current study are available from the corresponding author upon reasonable request.
The authors declare no competing interests.
Funding was not received from any organization, but APHI has covered data enumeration costs.
HA conceived the study, carried out the overall design, analyzed, and interpreted the data. NF, BB, AA, BB, MT, YB, and GM drafted the manuscript and revised it critically for important intellectual content and assisted with the development of the questionnaire and drafted the manuscript. All authors read and approved the final manuscript.
HA has MPH in Human Nutrition.